Hindu Temple Youth Group 2026-2027 Registration
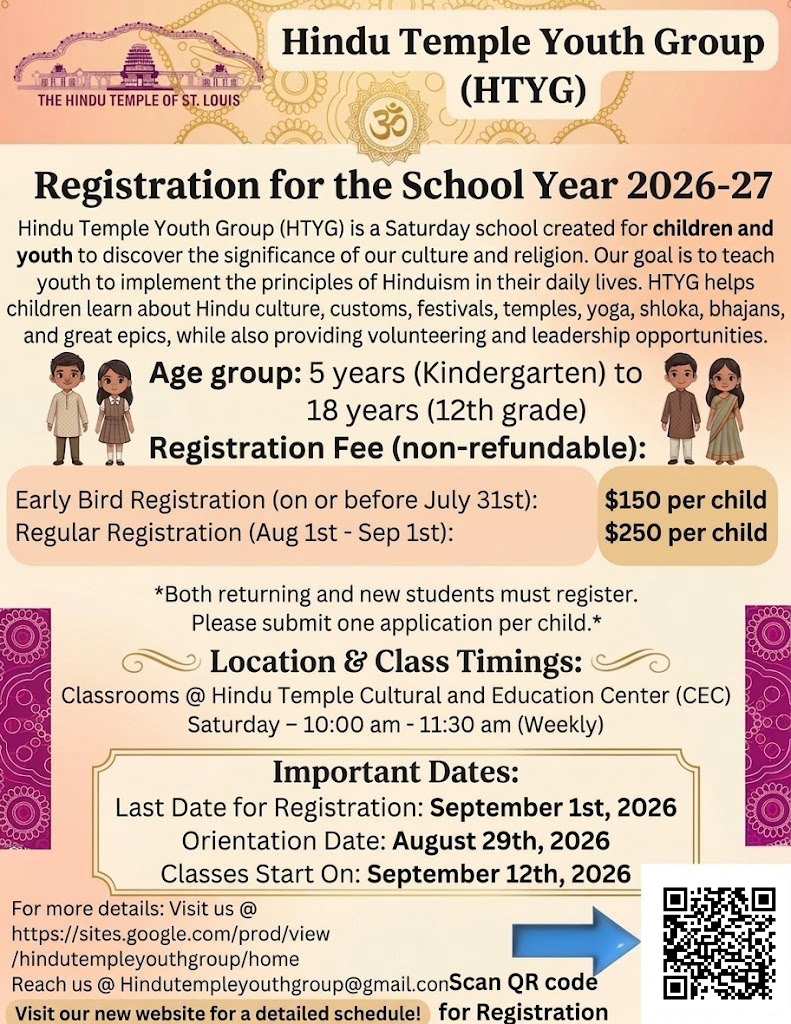
- Description
Dear Parents,
Please review the code of conduct:
Click here--> https://sites.google.com/prod/view/hindutempleyouthgroup/code-of-conduct
Please review the waiver form (This form can be signed during Orientation)
Hindu Temple of St. Louis – Youth Group
Participation Waiver and Release of Liability Form
Participant Information:
Name: _______________________________________
Age: _________ Date of Birth: ________________
Address: _____________________________________
City: ____________________ State: ____ ZIP: _______
Phone: ___________________ Email: ______________
Parent/Guardian Information (if participant is under 18):
Name: _______________________________________
Phone: ___________________ Email: ______________
Waiver and Release of Liability
I, the undersigned, understand and acknowledge that participation in activities, events, and programs organized by the Hindu Temple of St. Louis Youth Group (“Youth Group”) involves physical activities and the potential for risks and hazards that could result in injury or illness.
In consideration of being allowed to participate in any and all Youth Group activities, events, or programs, I hereby assume full responsibility for any risk of bodily injury, illness, death, or property damage arising out of or related to participation.
I further agree to release, indemnify, and hold harmless the Hindu Temple of St. Louis, its Board of Trustees, Youth Group coordinators, volunteers, employees, and agents from any and all liability, claims, demands, losses, or damages caused or alleged to be caused in whole or in part by the negligence or fault of the released parties.
This waiver applies to any transportation provided by the Youth Group or its volunteers for activities.
Medical Authorization
In the event of an emergency, I authorize the Youth Group leaders or temple representatives to obtain medical treatment for me/my child as deemed necessary. I understand that I am responsible for all medical costs incurred as a result of any injury or treatment.
Medical Conditions/Allergies (if any):
Emergency Contact Name: _________________________
Relationship: __________ Phone: __________________
Acknowledgement and Signature
I have read and fully understand this waiver, release of liability, and medical authorization, and I sign it voluntarily.
Signature of Participant (if 18 or older):
_____________________________________ Date: ___________
Signature of Parent/Guardian (if participant is under 18):
_____________________________________ Date: ___________